Understanding the High Risks of Placenta Previa Accreta in Patients with Macroscopic Hematuria
- Dr. Reena Sherene
- Jun 28
- 3 min read

Placenta previa accreta presents a significant challenge in obstetrics, especially when complicated by unusual symptoms such as macroscopic hematuria. This condition carries a high risk of severe bleeding and complex surgical management. Understanding its clinical presentation, imaging characteristics, and surgical findings is essential for healthcare professionals managing these high-risk pregnancies.
What Is Placenta Previa Accreta and Why It Matters
Placenta previa accreta occurs when the placenta implants abnormally low in the uterus, covering the cervix (placenta previa), and invades the uterine wall more deeply than usual (accreta). Instead of detaching normally after delivery, the placenta adheres firmly to the myometrium or even beyond, making separation difficult or impossible.
This abnormal attachment can lead to:
Severe bleeding during delivery
Increased risk of hysterectomy to control hemorrhage
Complications for both mother and fetus
When patients present with macroscopic hematuria—visible blood in the urine—this signals possible involvement of adjacent structures such as the bladder, indicating a more invasive form of placenta accreta (often termed placenta percreta). This symptom raises the stakes for diagnosis and surgical planning.
Imaging Findings: What Transabdominal and Transvaginal Scans Reveal
Ultrasound remains the primary imaging tool to evaluate placenta previa accreta. Both transabdominal and transvaginal scans provide critical information about placental location, depth of invasion, and vascularity.
Key ultrasound findings include:
Placental lacunae: These are irregular vascular spaces within the placenta that appear as multiple hypoechoic or anechoic areas. Their presence and number correlate with the severity of accreta. Lacunae often have turbulent blood flow on Doppler imaging, indicating abnormal vasculature.
Myometrial thinning: The myometrium beneath the placenta appears thin or absent, suggesting deep placental invasion. A myometrial thickness less than 1 mm is highly suspicious for accreta.
Increased vascularity: Color Doppler imaging shows abnormal blood flow patterns, including numerous large vessels crossing the uterine serosa and bladder interface. This vascularity signals potential placental invasion beyond the uterus.
Transvaginal ultrasound offers higher resolution images of the lower uterine segment and cervix, improving detection of placental attachment and invasion. Combining both approaches enhances diagnostic accuracy.
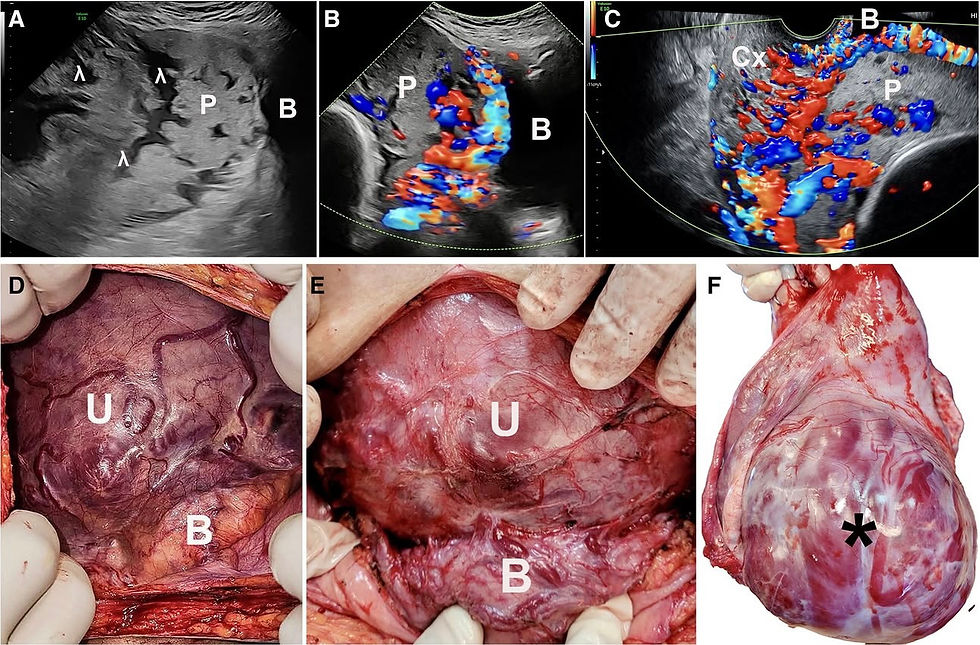
High risk of massive hemorrhage and hysterectomy in patients with placenta previa accreta presenting with macroscopic hematuria: A, Transabdominal scan showing placenta (P) previa covering the cervix containing several lacunae (1) and a large area (>50%) of myometrial thinning with a placental bulge (arrow) toward the bladder (B). B, Transabdominal scan with CDI mapping of the midline area showing increased subplacental and intraplacental vascularities. There is extreme myometrial thinning in both images. C, Transvaginal scan with CDI mapping showing the involvement of the cervix (Cx) with increased subplacental and intracervical vascularities. D,The anterior uterine (U) wall at laparotomy before dissection of the bladder (B) showing abnormally large vessels under the serosa. E, Same as (D) after partial dissection of the bladder from the uterine wall showing vascular anastomoses between the bladder and uterus. F,Hysterectomy specimen showing the dehiscent area (*) through which placental tissue can be seen.
Surgical Findings During Laparotomy
When imaging suggests placenta previa accreta with possible bladder involvement, surgical exploration via laparotomy is often necessary. The operation reveals the extent of placental invasion and guides management.
Typical findings include:
Abnormal vessels: Surgeons encounter numerous enlarged, tortuous vessels on the uterine surface and surrounding tissues. These vessels are fragile and prone to bleeding.
Vascular anastomoses: There may be direct connections between uterine vessels and bladder or pelvic vessels, complicating dissection and increasing hemorrhage risk.
Placental invasion beyond the uterus: In severe cases, the placenta penetrates the uterine serosa and invades the bladder wall, explaining symptoms like macroscopic hematuria.
These findings confirm the diagnosis and highlight the complexity of surgical management.
Risks and the Need for Hysterectomy
Placenta previa accreta carries a high risk of massive hemorrhage during delivery or surgery. Attempts to separate the placenta can cause life-threatening bleeding that is difficult to control.
To manage this risk, a hysterectomy—removal of the uterus—is often necessary. This procedure stops bleeding by removing the source but results in loss of fertility. Surgeons must prepare for:
Large-volume blood transfusions
Multidisciplinary involvement, including urology if bladder invasion is present
Intensive postoperative care
Early diagnosis and planning reduce complications but do not eliminate the inherent risks.
Summary and Clinical Takeaway
Placenta previa accreta is a dangerous condition that demands careful evaluation and management. In patients presenting with macroscopic hematuria, suspicion for placental invasion into the bladder or surrounding tissues must be high. Ultrasound imaging plays a vital role in identifying placental lacunae, myometrial thinning, and abnormal vascularity, guiding surgical planning.
Surgical findings often reveal complex vascular networks and placental invasion beyond the uterus, necessitating hysterectomy to control bleeding. Awareness of these risks helps clinicians prepare for potential complications and improve maternal outcomes.
Reference:
AJOJ: High risk of massive hemorrhage and hysterectomy in patients with placenta previa accreta presenting with macroscopic hematuria



Comments