ABNORMAL UTERINE BLEEDING MANAGEMENT- FOGSI
- Dr. Reena Sherene
- 4 days ago
- 2 min read

AUB MANAGEMENT IN PERIMENOPAUSE - FOGSI
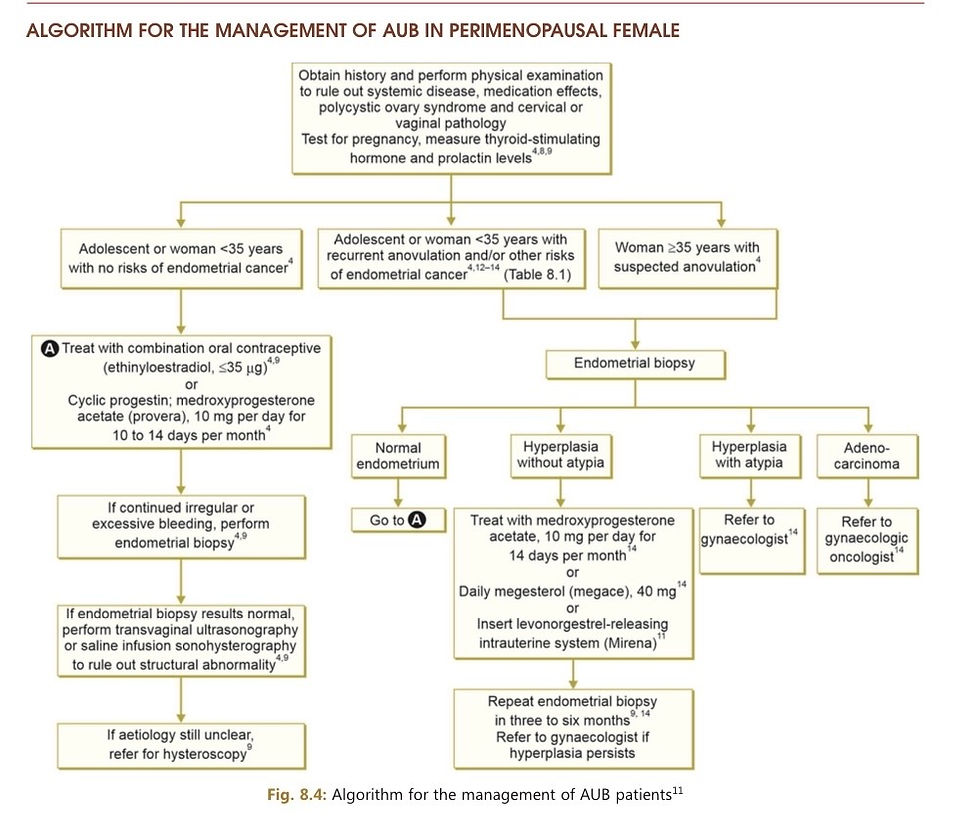
The medical management of Abnormal Uterine Bleeding (AUB) according to FOGSI (Federation of Obstetric and Gynaecological Societies of India) guidelines is categorized into managing acute heavy episodes vs. long-term treatment. Treatment is tailored based on patient age, fertility desires, and underlying causes (using the PALM-COEIN classification).
1. Acute Heavy AUB (Immediate Control)
For active, heavy bleeding, the goal is to stabilize the patient and stop the bleeding rapidly.
High-Dose Hormonal Therapy: Oral progestins (e.g., medroxyprogesterone acetate 20mg three times daily, or norethisterone acetate 10 mg three times daily) or multidose Combined Oral Contraceptives (COCs) (e.g., 30mug ethinylestradiol, two pills every 12hours for 5days).
Antifibrinolytics: Tranexamic acid is used adjunctively to reduce blood loss.
Antiemetics: May be co-prescribed to manage nausea associated with high-dose hormones.
2. Long-Term Medical Management
Management of chronic AUB focuses on regulating cycles, reducing menstrual blood loss, and addressing specific underlying causes (e.g., fibroids, adenomyosis, coagulopathies).
Levonorgestrel-Releasing Intrauterine System (LNG-IUS): Highly recommended by FOGSI as a first-line treatment for heavy menstrual bleeding and AUB caused by adenomyosis (AUB-A) or fibroids (AUB-L), particularly for fertility preservation.
Combined Oral Contraceptives (COCs): Recommended for regulating cycles, treating ovulatory dysfunction, and providing symptomatic relief.
Oral Progestogens: Can be used cyclically (e.g., days 15-25 of the cycle) for women who do not require contraception but need endometrial protection.
GnRH Agonists: Often used as second-line therapy for adenomyosis or large fibroids, usually given with "add-back" therapy (low-dose estrogen/progestin) to prevent bone mineral density loss.
Non-Hormonal Therapies: NSAIDs and tranexamic acid are excellent options for women who want to avoid hormones but require relief from heavy flow or dysmenorrhea.
Note: In structural causes (like large submucosal fibroids or polyps) or when medical management fails, surgical interventions (such as myomectomy, endometrial ablation, or hysterectomy) are considered.
AUB is one of the most common causes (70%) detected in the gynaecological presentation in perimenopausal women.
In perimenopausal women with AUB, TVS-USG should be the investigation of choice due to its convenience, accuracy and non-invasiveness. In patients with hyperplastic endometrium and/or endometrial thickness greater than 8 mm, a histopathological study of the endometrium is warranted to rule out atypical changes or endo- metrial malignancy
Dilatation and curretage is diagnostic tool for patients with AUB.
• The primary indication for invasive methods like
D and C should be in cases with abnormal thickness of endometrium >8 mm in order to obtain endometrial tissue to exclude precancerous lesion or endometrial cancer.
• Anaemia,andhypovolaemiacanresultinextreme conditions of significant blood loss.
• Endometriosis should be taken into consideration for one of the causes of AUB. This can help in removing major medical line of treatment.
Surgeryshouldbethelastsourceoftreatmentunless we have a strong reason to do so. (Some uterine bleed- ing can be managed with first-line of treatment.)
Therapeuticdecisionsshouldbetakenconsidering patient’s well-being.
Manytherapeuticmodalitiesleadtoasimilarout- come, so be sure to discuss the risk, benefits and alternatives of available options
#OBGYN #GYNECOLOGIST #OBGYNRESIDENT #FERTILITYDOCTOR #GYNAECOLOGY #AUB



Comments